Penile Abnormalities

Male Tanner stages, from Campbell's
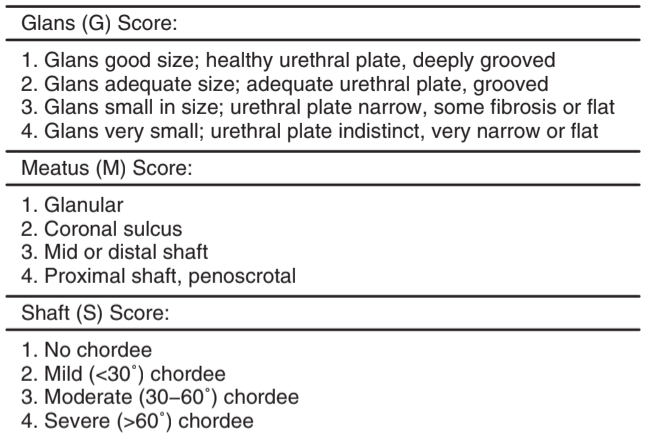
Glans Meatus Shaft score, assessed at time of surgery, from Campbell's
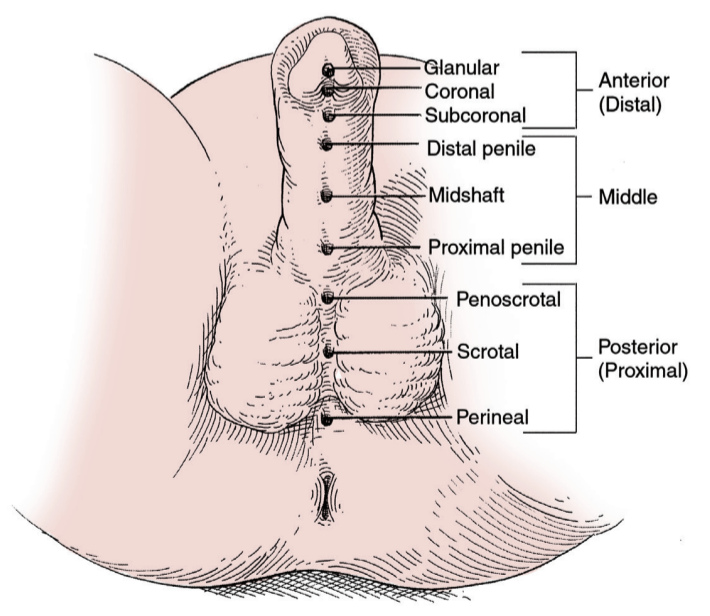
Variation in hypospadias location, from Campbell's
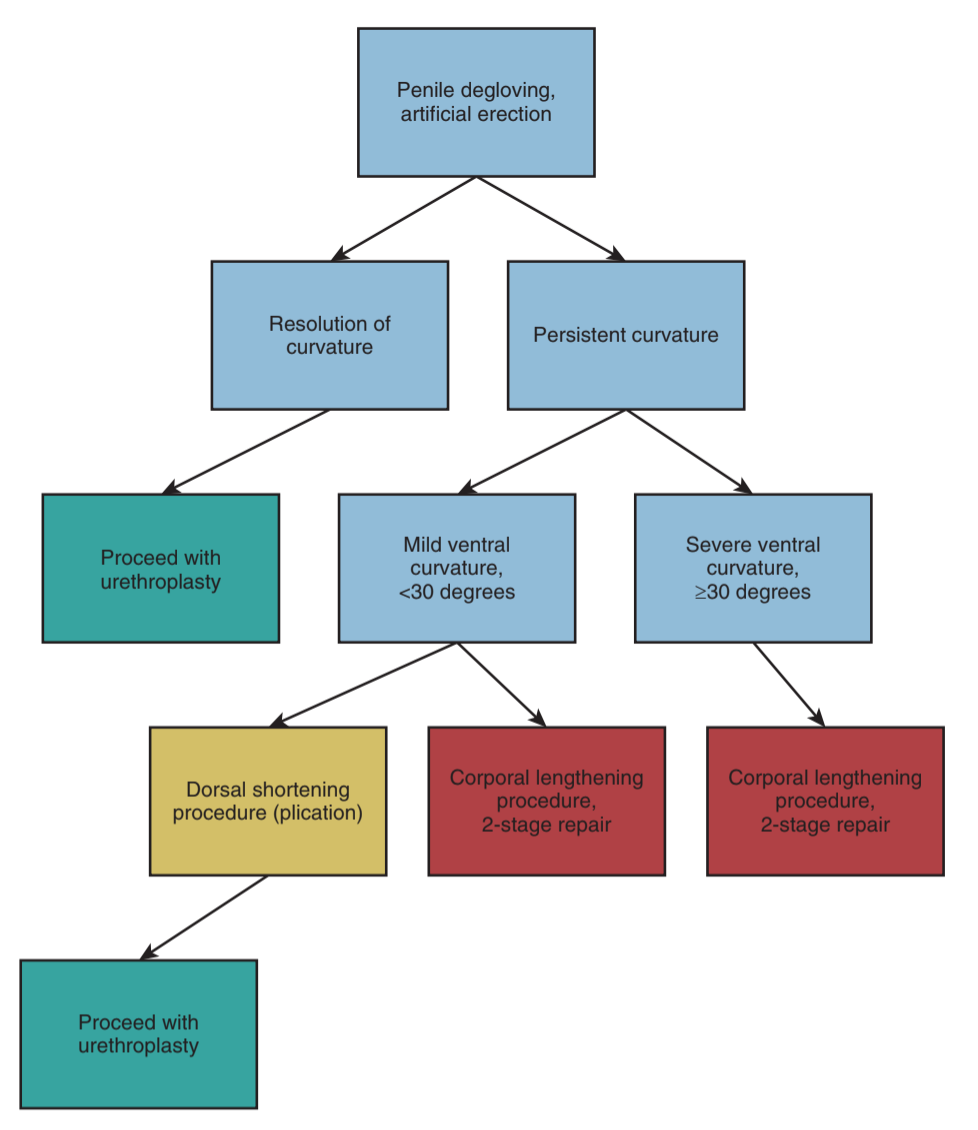
Management of penile curvature after intraoperative degloving, from Campbell's
Phimosis
- Physiologic at birth, separates over time due to smegma production and intermittent erections
- Foreskin easily retractable in 90% by 3yo and > 99% by 17yo
- Avoid forceful foreskin retraction, can cause scarring and pathologic phimosis
- Circumcision indications: persistent or secondary phimosis, balanitis, posthitis, BXO, recurrent UTIs
- Balanitis Xerotica Obliterans (BXO): can treat with steroids or circumcision, may require reconstruction if meatus involved, 20% meatal recurrence
- Steroids: apply topical betamethasone 0.05% BID-TID with gentle manual retraction, usually responds within 2-8 weeks (50-90% success) but often regress once treatment stopped
- For details on circumcision technique and considerations, see separate section
Paraphimosis
- Can cause glans gangrene if not reduced
- Conservative treatments: manual compression (with coban), iced glove for 5 minutes
- Next steps: perform penile block, consider puncturing holes in edematous foreskin
- Last steps: may require dorsal slit or circumcision for treatment
Hypospadias
Evaluation/Considerations
- Exam Triad: ectopic ventrally located meatus, ventral penile curvaturee, incomplete dorsally hooded foreskin
- Associated conditions: hydrocele/hernia (9%), and cryptorchidism (9-30%)
- DSD testing: obtain US, karyotype, hormone labs if undescended testis or micropenis in the setting of proximal hypospadias
- Megameatus intact prepuce: <1% hypospadias, normal foreskin, meatus anomaly only noted when attempting circumcision, does not require repair (but can be offered)
- Prostatic utricle: often enlarged, can make catheterization difficult, may need coude
- Imaging: usually not required, but renal/bladder US recommended if multiple other congenital anomalies
The Inconspicuous Penis
- Buried penis: normal penis hidden under fat pad, due to obesity/scarring, can treat depending on cause with weight loss or scar repair, avoid reconstruction until puberty due to potential normal loss of fat pad during puberty
- Webbed penis: scrotal skin extends onto ventral penis, can repair by fixing skin to ventral penile base, occasionally may require ventral repair of hypoplastic distal urethra
- Micropenis: > 2.5 SD below average stretched length for age, obtain karyotype and serum T if diagnosed at birth, can attempt treatment with short course of testosterone
Penile Masses
- Evaluation: assess duration, location, prior surgeries, and changes in size to help determine origin
- Parameatal urethral cyst: rare, excise cyst, avoid meatal stenosis
- Median raphe cyst: epidermal cyst, can observe if asymptomatic, otherwise can resect
- Inclusion cyst: occur due to epithelium within subQ tissue, seen after penile surgery
- Congenital nevus: superficial and benign, but should be removed
- Juvenile xanthogranulomas: benign and self-limiting, pigmented nodules 2-20mm, firm/rubbery, can observe to avoid surgery
Miscellaneous
- Aphallia: rare (1 per 10-30mil), absent penile shaft with anteriorly displaced anus, usually associated with other GU abnormalities, assess karyotype
- Diphallia: rare (1 per 5mil), spectrum of presentation and associated GU conditions, obtain RUS and VCUG
- Lymphedema: can observe, but may require removal of all affected tissue and placement of graft/flap
- Neonatal priapism: spontaneously resolves in 2-6 days without treatment
- Balanoposthitis: inflammation usually from fungal or irritative source, treat with topical steroid and antifungal cream, usually no PO meds required, consider further workup if symptoms persist
- Hypospadias, chordee, and torsion: see separate surgery page
References
- AUA Core Curriculum
- Baskin, Laurence S. Handbook of pediatric urology. Lippincott Williams & Wilkins, 2018.
- Long, C., M. Zaontz, and D. Canning. "Hypospadias." Campbell-Walsh Urology 12 (2020).
- Palmer, L., and J. Palmer. "Management of Abnormalities of the External Genitalia in Boys." Campbell-Walsh Urology 12 (2020).