Upper Tract Trauma
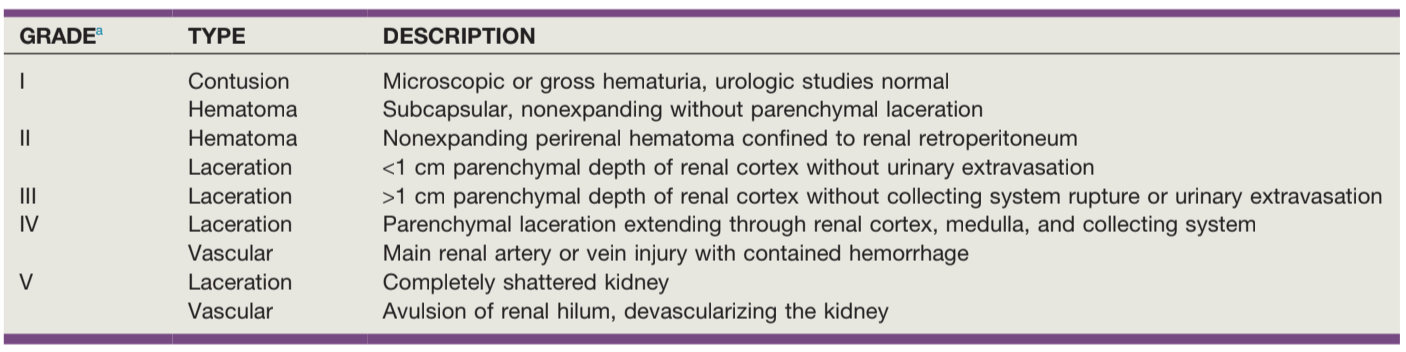
AAST renal injury severity, from AAST + Campbell's
Renal Trauma
| IF... | THEN... | |
|---|---|---|
| Diagnosis | Blunt trauma + GH | Obtain CTU |
| Blunt trauma + MH + SBP < 90 | ||
| Blunt trauma concerning for renal injury but no hematuria | ||
| Penetrating trauma near kidney with(out) hematuria | ||
| Exam (rib fx, flank bruising) concerning for renal injury | ||
| Unstable patient taken to OR without imaging | Obtain on table IVP 2mL/kg contrast bolus XR 10-15min later |
|
| MH, no hypotension, no concerning injury | Can observe without imaging | |
| Management | Grade I-III injury | Manage conservatively |
| Grade IV-V injury | Repeat CT within 48hrs | |
| Fever | ||
| Worsening flank pain | ||
| Worsening anemia | ||
| Abdominal distension | ||
Expanding urinoma with:
|
Provide GU drainage Stent preferred Can consider PCN or drain |
|
| Urinary extravasation without above signs | Can manage conservatively | |
| Hemodynamically unstable not responding to resuscitation | Absolute indication for embolization/exploration | |
| Hemodynamically unstable + perirenal hematoma > 4cm or Grade 3-5 injury with contrast extravasation | ||
| Expanding/pulsatile renal hematoma | ||
| Suspected vascular pedicle avulsion | ||
| UPJ avulsion | ||
| Urine extravasation with significant parenchymal devascularization | Relative indication for embolization/exploration | |
| Renal + colon/pancreas injuries | ||
| Arterial thrombosis | ||
| Urine extravasation from parenchymal injury |
CT findings concerning for major renal injury (9x more likely to require intervention)
- Medial hematoma: suggests vascular injury
- Medial urinary extravasation: suggests renal pelvis or UPJ avulsion
- Global lack of parenchymal enhancement: suggests renal artery occlusion
- Combination of 2+: large hematoma > 3.5cm, medial renal laceration, vascular contrast extravasation
Post-renal injury hypertension mechanisms (renin production stimulated by partial ischemia)
- Goldblatt kidney: renal artery injury leading to stenosis/occlusion
- Page kidney: compression of renal parenchyma with blood/urine
- Arteriovenous fistula: decreased renal perfusion due to diversion
Renal injury tips
- Prevalence: up to 34% have renal injury without hematuria or hypotension
- Venous injury: CT is not sensitive, have high suspicion in presence of medial hematoma
- Intraoperative IVP: confirms presence of contralateral kidney prior to performing trauma nephrectomy
- Embolization failure: seen in 13-88%, can repeat embolization
- Pseudoaneurysm: may develop in up to 2.5% renal trauma
- Fluid collections: urinoma (0-20 HU, delayed contrast pooling), hematoma (> 30 HU), abscess (rim enhancement + > 20 HU with contrast)
- During exploration, isolation/control of renal vessels prior to renal exposure no longer necessary
- Surgery tips: can attempt renal repair with debridement, suture ligation, closing collecting system and parenchymal defects, flaps, and drain placement
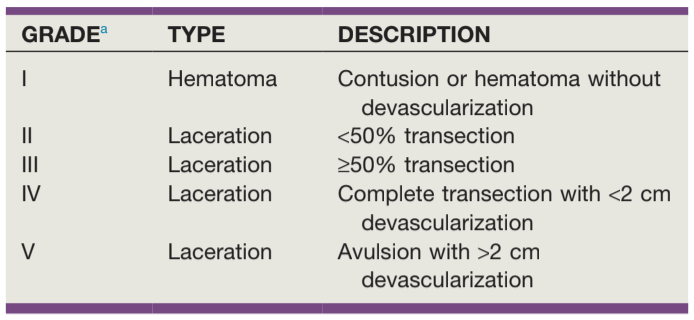
AAST ureteral injury severity, from AAST + Campbell's
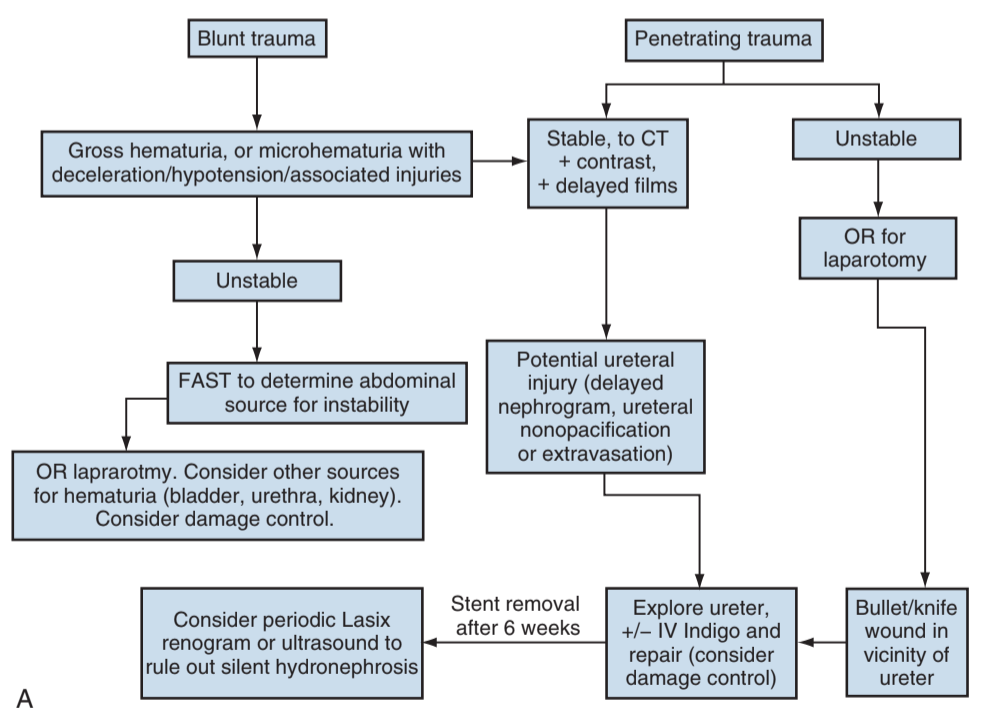
Algorithm for ureteral injury from external trauma, from Campbell's
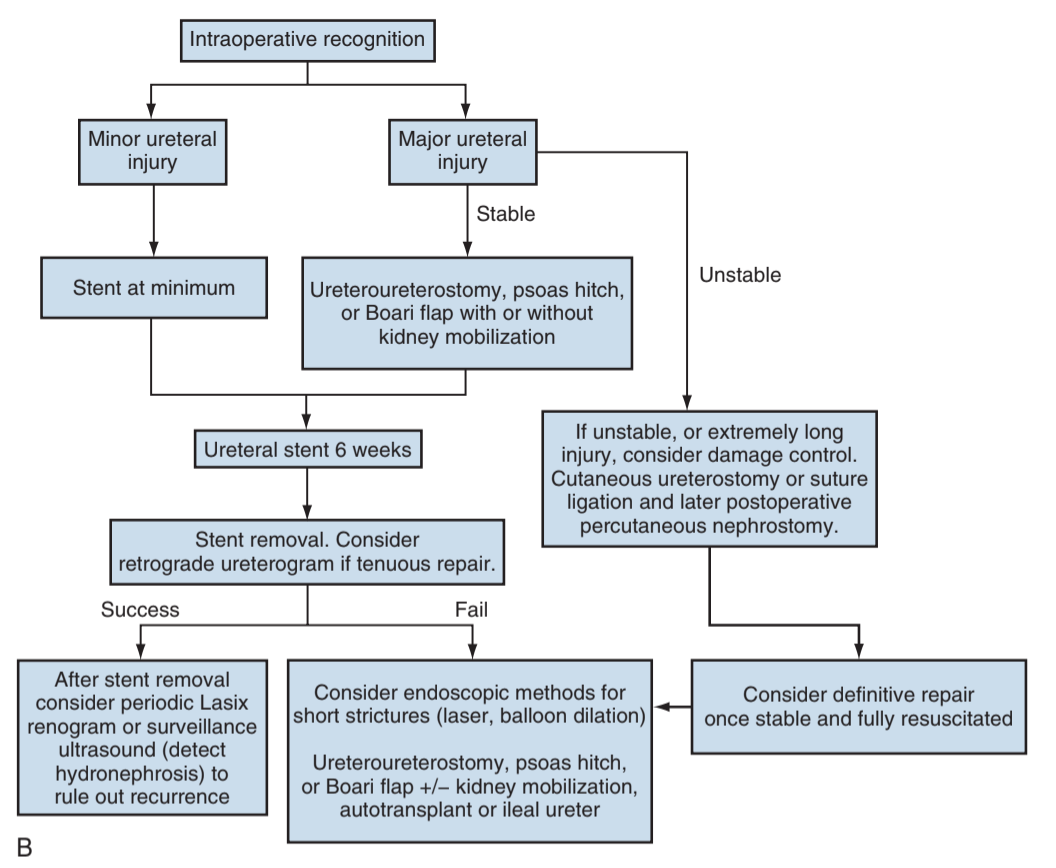
Algorithm for iatrogenic ureteral injury discovered intraoperatively, from Campbell's
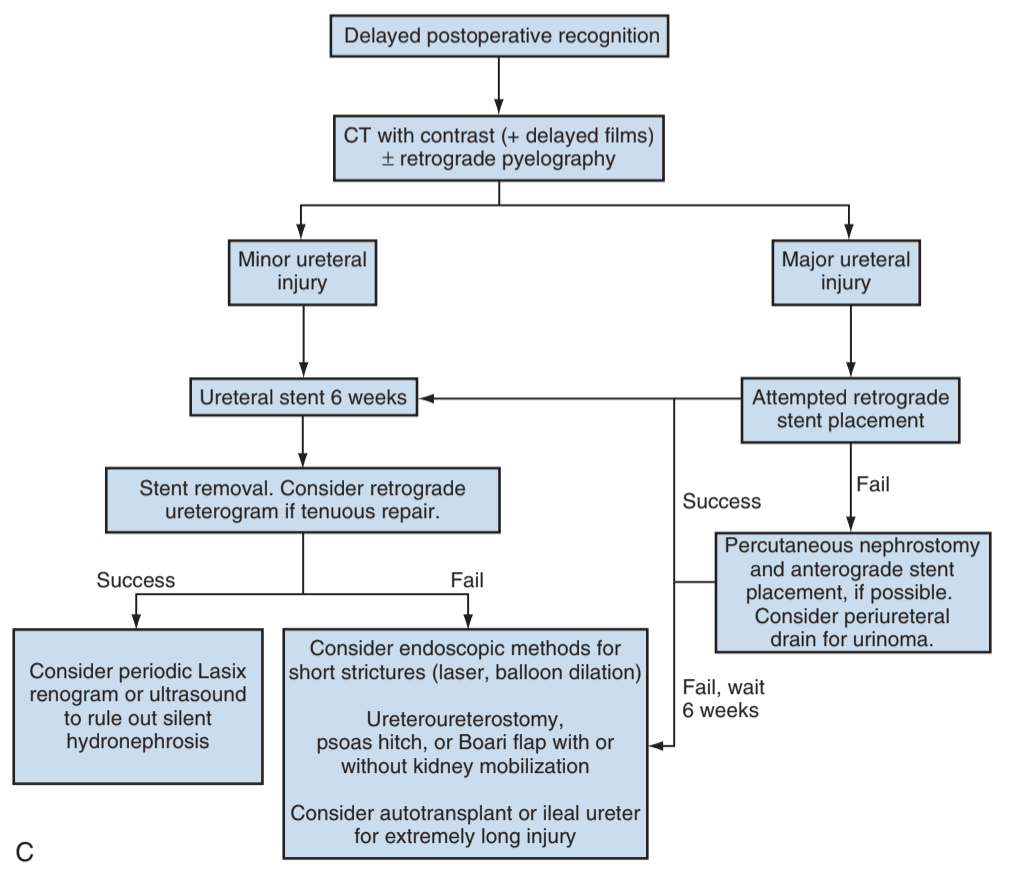
Algorithm for iatrogenic ureteral injury discovered postoperatively, from Campbell's
Ureteral Trauma
| IF... | THEN... | |
|---|---|---|
| Diagnosis | Ureteral injury suspected (see renal criteria) | CT urography |
| Assessing for intraoperative injury | Inspect ureter Inject dye IV or via renal pelvis Contrast evaluation |
|
| Management | Stable + contusion or crush injury | Place stent Debride if large injury |
| Stable + intraop laceration | Place stent Repair laceration |
|
| Unstable + intraop injury | Ligate ureter with nonabsorbable stitch Place PCN or cutaneous ureterostomy +/- stent Delayed repair |
|
Delayed identification:
|
Retrograde pyelogram + stent placement If fails, place PCN Delayed repair |
|
| Ureterovaginal fistula | Stent (64-76% success) Delayed repair (100% success) |
Prophylactic stenting
- Does not decrease risk for injury, but improves chances of identifying injury
- Anuria risk with bilateral stents: 1-5% (place over a wire to minimize trauma)
- Ureteral injury during placement: 1%
- Inability to place stent: 13% unilateral, 2% bilateral
Ureteral repair principles
- Avoid ureteral devascularization
- Minimize debridement but assess for vascularity
- Perform spatulated, tension-free, stented, watertight anastomosis
- Close peritoneum if possible
- Place drain to evaluate for leak
- Do not tunnel ureteroneocystotomies
- Consider omental flap for severe injuries
Ureteral injury tips
- Remove catheter, then drain, to prevent urinoma formation
- Either repair immediately or delay repair for 6-8 weeks due to inflammation
- Distal injuries may require reimplantation
- Endoscopic iatrogenic injuries may heal with stenting alone
- Absence of hematuria and presence of bilateral jets is a poor predictor of injury, but can consider visualizing efflux of dye for confirmation
References
- Brandes, S. and J. Eswara. "Upper Urinary Tract Trauma." Campbell-Walsh Urology 12 (2020).
- Morey, Allen F., et al. "Urotrauma Guideline 2020: AUA Guideline." The Journal of Urology 205.1 (2021): 30-35.
- Wieder JA: Pocket Guide to Urology. Sixth Edition. J.Wieder Medical: Oakland, CA, 2021.