Peyronie Disease
Evaluation + Workup
History
- Symptoms: pain, deformity, palpable plaque, and erectile dysfunction
- ED vs PD: ask, "if your penis was straight with the same quality of rigidity you have now, do you think it would be adequate for penetrative sexual activity?", ED treatments unlikely to cause Peyronie, but more likely to expose patients who would otherwise not notice
- Assess ED risk factors: DM, HTN, HLD, smoking
- Resolution:50% see worsening curvature 12-18 months after presentation, 13% or less see some improvement
- Risk factors: prior trauma, sexual microtrauma, DM, low T, smoking, alcohol, ED, associated with depression, anxiety, and other psychosocial issues, some association with Dupuytren disease (hand/foot contractures)
- Questionnaire: assess severity with the PDQ (PDF here)
Exam and adjuncts
- Ask to bring picture from home of erection from above and from the side
- Exam: examine penis on stretch and palpate for plaques, can use goniometer to accurately measure curvature severity
- Stretched penile length: pubis to corona dorsally
- Further testing: no benefit to US or lab evaluation
- Intracavernosal injection: recommended to perform in-office prior to any invasive therapies
- congenital penile curvature (CPC): important to differentiate, shows smooth curvature on exam without plaques
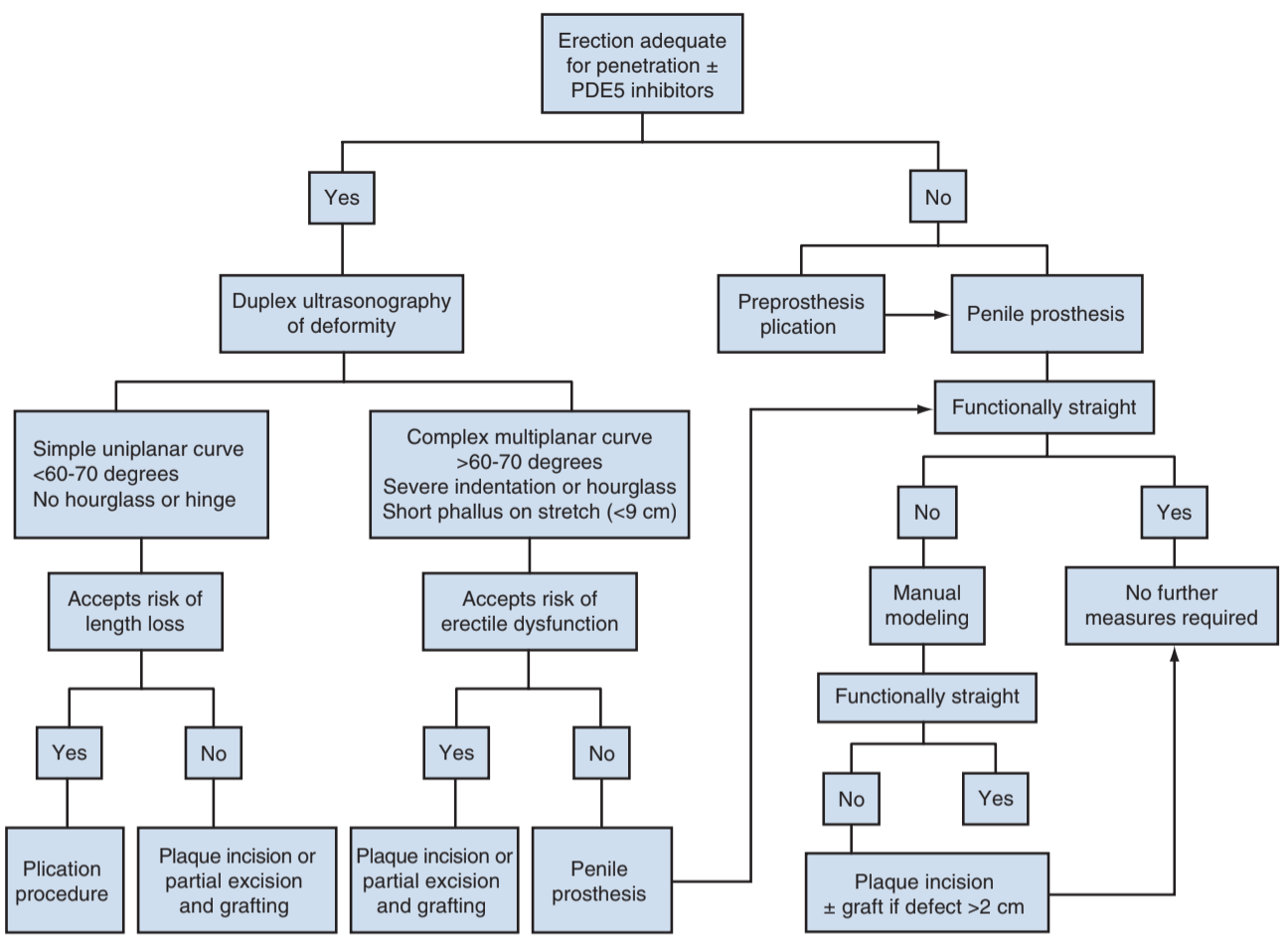
Peyronie treatment algorithm, from Campbell's
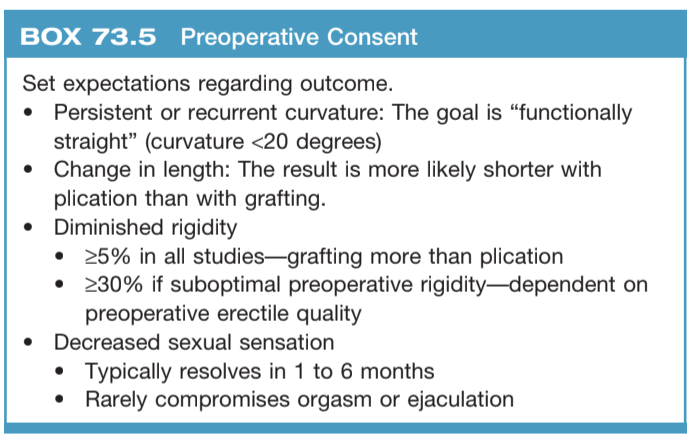
Peyronie consent tips, from Campbell's
Nonsurgical options
Xiaflex
- Xiaflex (collagenase Clostridium histolyticum): proven to improve curvature, side effects include bruising (80%), swelling (55%), pain (45%), hematoma (3.7%), penile fracture (0.4-1.5%)
- Xiaflex technique: inject two dose (1-3d apart), then in-office modeling (grasp 1cm proximal and distal, bend opposite curvature x30s x3), perform up to 4 cycles, 6wk between cycles, stop once curvature < 15deg
- IMPRESS trial: 8 injections 0.58mg CCH with modeling, 34% average improvement
- Collagenase penile fractures: manage conservatively, likely to heal, hard to repair surgically due to poor tissue quality
Other options
- Intralesional verapamil: unclear dosing and frequency, some proven treatment benefit, side effects include bruising, dizziness, nausea, pain
- Intralesional IFN-a: can offer (per guidelines), side ffects include sinusitis, flu symptoms, penile swelling
- Other options:ral agents, topical agents, XRT, and shock wave therapy have not been shown to provide a treatment benefit
- Traction: small improvement in curvature and length, 85% satisfaction, need to wear for 3+hr daily
- Acute setting: manage pain with NSAIDs
Surgical options
General info
- Indications: inability to have satisfactory intercourse, pain to self or partner, or distress due to appearance
- Timing: wait until at least 3-6mo after initial symptoms and pain has resolved
- Consent: penile shortening, decreased sensation, decreased rigidity, persistent curvature, appearance
- Postop care: avoid intercourse for 4-6 weeks, can perform massage/stretching (unclear benefits), consider traction if tolerable
Shortening
Grafting
- Indications: better choice for severe curvature or hourglass deformity but more likely to result in inadequate erections
- Options: excision has higher rate of postop ED, incision is preferred
- Graft choices: can use autologous (penile vein, saphenous vein, fascia lata, rectus fascia), allografts (human pericardium), xenografts (bovine pericardium), or synthetic (gortex, dacron)
- Success: fixes curvature in > 80%, > 70% satisfaction
ED + PD
- Indications: if ED in presence of PD, treat ED w/ IPP and intraop grafting/plication
- Maximal modeling: maximally inflate cylinders, bend penis in direction opposite plaque x90s, can inflate more, may feel plaque "crack"
- Side effects: biggest patient concern is postoperative loss of length, urethral injury occurs 2-3% during modeling
References
- AUA Core Curriculum
- Nehra, Ajay, et al. "Peyronie’s disease: AUA guideline." The Journal of urology 194.3 (2015): 745-753.
- Seftel, A. and H. Yang. "Diagnosis and Management of Peyronie's Disease." Campbell-Walsh Urology 12 (2020).
- Wieder JA: Pocket Guide to Urology. Sixth Edition. J.Wieder Medical: Oakland, CA, 2021.