Urinary Tract Infections
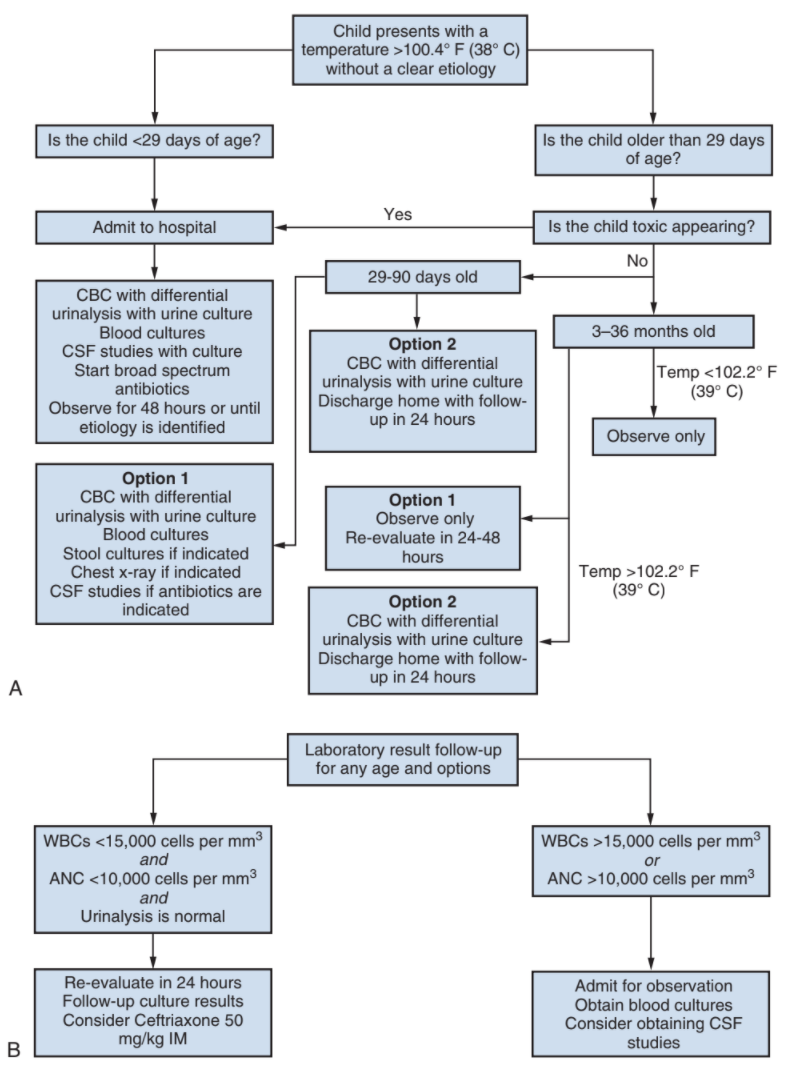
Workup with fever without obvious cause, from Campbell's
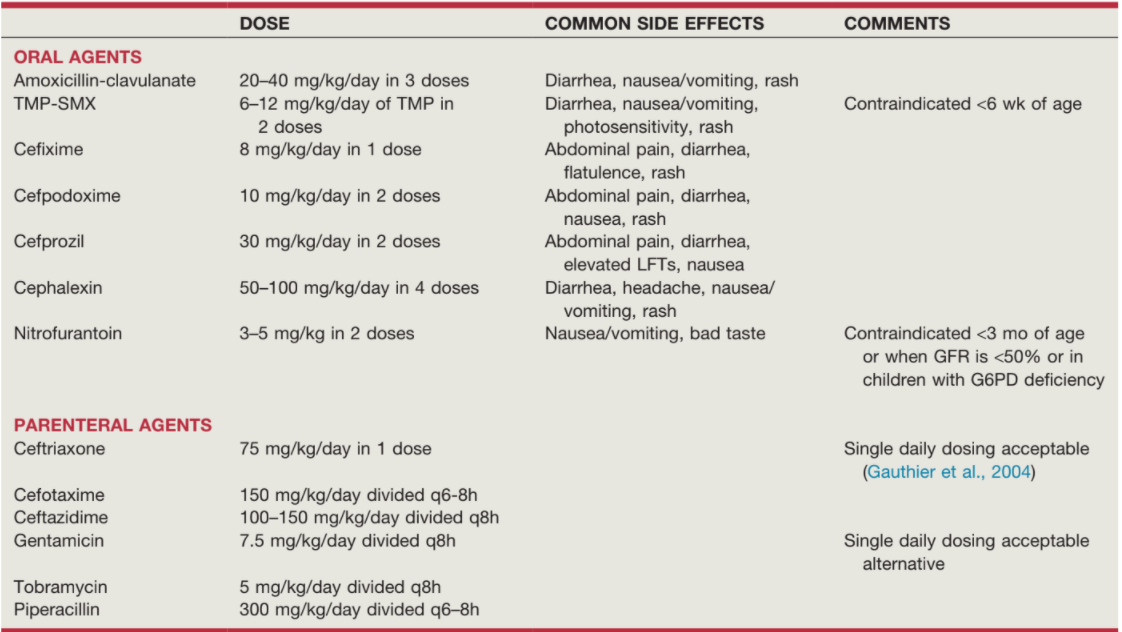
Pediatric antibiotic dosing, from Campbell's
Evaluation
General considerations and risk factors
- UTI is cause of 7% febrile infections in infants, 8% if > 24mo
- Bacteremia present in 7-13% with fever
- If < 24mo, fever > 40, hx UTI, SP tenderness, and uncircumcised penis are most predictive of UTI in a febrile child
- Age/gender: 2.7% boys vs 0.7% have a UTI during 1st year, then 0.03%-0.2% boys vs 1-3% girls per year after 1st year
- Circumcision in 1st 6mo of life decreases rates x10 - 111 otherwise-normal boys need to be circumcised to prevent one UTI, but only 11 if hx UTI, only 4 if hx high grade VUR
- Other risk factors: vesicoureteral reflux, neurogenic bladder, bowel/bladder dysfunctoin
Imaging for UTI
- Renal US: obtain if febrile UTI, < 6mo, or > 6mo and atypical UTI
- VCUG: obtain if abnormal RUS, 2+ febrile UTI, UTI in circumcised boy, or abnormal UTI, can perform as soon as asymptomatic and urine is sterile, cycling study recommended (more sensitive)
- DMSA scan: consider if atypical UTI, may need to wait 1-2yrs to assess scarring
Treatment
Treatment considerations
- Indications for inpatient management: age < 1mo (some say < 2-6mo), toxic appearance, not tolerating PO intake, concerns for antibiotic compliance
- Consider renal US if no improvement within 48hrs
- Duration: treat for 7-14 days, longer for severe infections
- Age considerations: avoid TMP/SMX if < 6 weeks, avoid nitrofurantoin if < 3mo
Other Infections
- Viral cystitis: more common in immunosuppressed situations, can have 50-80% mortality rate without treatment
- Funguria: more common with catheterization or prior antibiotic therapy, consider imaging to assess for fungal balls
Antibiotics for UTI
| Antibiotic | Dosing | N/V/D | Rash | Other side effects |
|---|---|---|---|---|
| Nitrofurantoin | 3-5mg/kg/d, BID | Yes | No | Hyperbilirubinemia if given < 3mo old |
| TMP/SMX | 8-10mg/kg/d (trimethoprim), BID | Yes | Photosensitivity | |
| Augmentin | 20-40mg/kg/d, TID | No | ||
| Cephalexin | 50-100mg/kg/d, QID | Headache, diarrhea | ||
| Cefprozil | 20mg/kg/d, BID |
References
- AUA Core Curriculum
- Baskin, Laurence S. Handbook of pediatric urology. Lippincott Williams & Wilkins, 2018.
- Cooper, C. and D. Storm. "Infection and Inflammation of the Pediatric Genitourinary Tract." Campbell-Walsh Urology 12 (2020).
- Peters, C., et al. "Management and Screening of Primary Vesicoureteral Reflux in Children: AUA Guideline." (2010).