Benign Prostatic Hyperplasia
Treatment of LUTS, from Campbell's
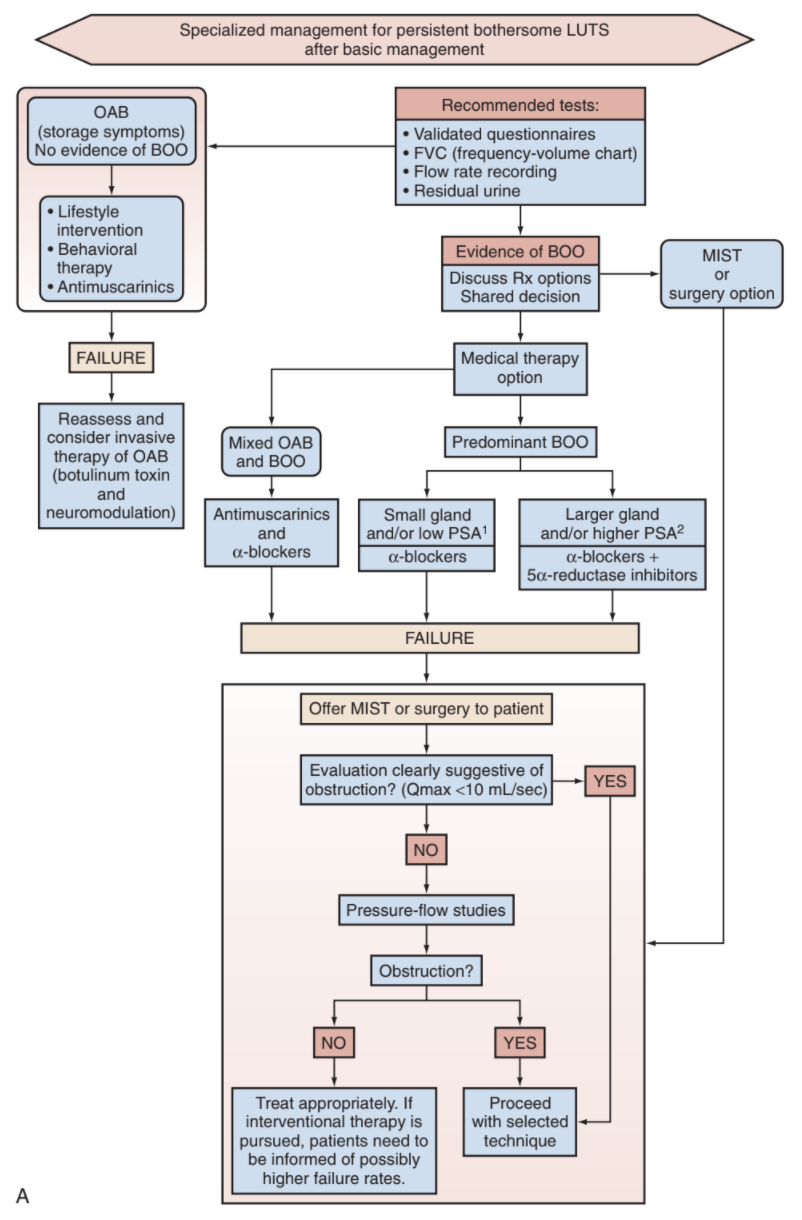
Non-Surgical Managment
Common BPH drugs
| Drug | Dosing | Uro-Selective? | Titration? | Side effects |
|---|---|---|---|---|
| Terazosin (Hytrin) | 2-5mg QHS | No | Yes | dizziness (14-17%), asthenia (5-13%) headache (5-13%), hypotension (2%) |
| Doxazosin (Cardura) | 2-8mg QHS | dizziness (5%), headache (5%) | ||
| Alfuzosin (Uroxatral) | 10mg QHS | No | dizziness (12%), asthenia (5%), hypotension (3%), CV effects (10%) | |
| Tamsulosin (Flomax) | 0.4-0.8mg QHS | Yes (a1A) | dizziness (3-15%), asthenia (24%), headache (5-16%), retrograde ejaculation (1-18%), CV effects (9%) | |
| Silodosin (Rapaflo) | 8mg QHS | retrograde ejaculation (10-14%), dizziness (8%), headache (3%) | ||
| Finasteride (Proscar) | 5mg daily | Type 2 | decreased libido (4-5%), ejaculatory dysfunction (4%), erectile dysfunction (6%), gynecomastia/breast tenderness (0.5-1%), cardiac failure (1%) | |
| Dutasteride (Avodart) | 0.5mg daily | No (Type 1 + 2) | ||
| Tadalafil (Cialis) | 5mg daily | Yes | No | headache (13%), dyspepsia (7%), flushing (7%) |
| Mirabegron (Myrbetriq) | 25-50mg daily | No | No | nasopharyngitis (3-6%), headache (2-3%), hypertension (10-12%) |
| Vibegron (Gemtesa) | 75mg daily | No | No | nasopharyngitis (3-6%), headache (2-3%) |
Conservative Management
- Watchful waiting: reasonable for mild symptoms, check symptoms annually
- Fluids: maintain 1.5-2L intake (adjust as needed), decrease caffeine/alcohol
- Nocturia prevention: restrict fluids 2-4hrs before bed, elevate legs if edema present, avoid evening diuretics
- Behavioral: timed voiding, double voiding, "urethral milking" (for postvoid dribbling)
- Constipation: avoid
Alpha-blockers
- Mechanism: a-receptor blockade leads to smooth muscle relaxation at bladder neck, prostate, and proximal urethra
- Receptor subtypes: a1A found in prostate/bladder neck smooth muscle, a1B found in blood vessels, a1D found in nasal passages, bladder, and spinal cord
- Effects: improves symptom scores by 30-40% and uroflow parameters by 20-25%, no effect on prostate size or PSA
- CV effects: alfuzosin increases CV effects, whereas tamsulosin/silodosin do not interact with cardiac medications
- Sexual effects: no proven effect on erectile function or libido, but tamsulosin/silodosin cause retrograde ejaculation and orgasmic impairment in ~17%
- Intraoperative floppy iris syndrome (IFIS): occurs during cataract surgery after a-blocker exposure, can occur even after drug discontinuation, tamsulosin (30-88%), alfuzosin (15-70%), doxazosin (2-45%)
5a reductase inhibitors
- Mechanism: prevents conversion of T to DHT, inhibiting prostate growth
- Effects: reduces prostate volume 20-25%, improves flow rate by 10%, improves symptom scores 20-30%, decreases urinary retention risk 50%, reduces need for prostate surgery 50%, decreases PSA 50%, decreases recurrent hematuria risk, takes 6 months for full effect
- Indications: prostate > 30g and PSA > 1.5
- Prostate cancer risk: potentially increases high-risk prostate cancer, although actual effect unclear
Anticholinergics
- Mechanism: antagonism of bladder muscarinic receptors results in bladder relaxation, decreasing bladder spasms
- Effects: reduces stoarge symptoms, increases PVR by an average of 25mL, < 3% retention risk
- Indications: most beneficial in patients with high storage symptom scores, high flow rate (> 5mL/s), low PVR (< 200mL), no hx retention
- Options: darifenacin 7.5-15mg QD, fesoterodine 4-8mg QD, oxybutynin IR 2.5-5mg 3-4x daily, oxybutynin ER 5-15mg QD, solifenacin 5-10mg QD, trospium 60mg QD or 20mg BID
- Side effects: dry mouth (≥ 16%), constipation (≥ 4%), dizziness (≥ 5%), and cognitive dysfunction
B3-Agonists
- Mechanism: stimulates bladder relaxation
- Dosing: mirabegron 25-50mg daily, vibegron 75mg daily
- Effects: reduces storage symptoms, increases PVR by average 30mL
Phosphodiesterase Type 5 inhibitors
- Mechanism: may increase oxygenation of tissue, relax bladder neck and prostate smooth muscle, decrease stromal proliferation and inflammation
- Effects: symptom score improvement 20-30%, may also improve flow rate, usually improves within 1 week but can take up to 2mo
- Tadalafil 5mg is currently the only option recomended for LUTS
Phytotherapy
- Different extracts and preparations have widely variable amounts of "active" ingredients
- Efficacy: all evidence is based on in vitro studies, no good long-term clinical evidence exists that phytotherapy is beneficial
- Common types: saw palmeto, African plum tree, stinging nettle, pumpkin seed, African star grass, rye grass pollen
Surgical Management
Indications for Surgery
- Hematuria: finasteride has proven benefit for decreasing further episodes, confirm BPH as cause with hematuria workup, can consider BPH surgical management at time of clot evacuation
- Bladder stones: can consider medical management after removal of bladder stones
- Recurrent UTIs: may be secondary to incomplete emptying
- Urinary retention: idiopathic vs iatrogenic, up-front surgery not recommended, 60% pass first voiding trial, up to 80% have another retention episode within 6 months
- Upper tract injury: not necessary to screen prior to interventions, if secondary to BOO then place catheter and reassess, bladder wall hypertrophy may cause persistent obstruction and require stenting
- Bladder diverticulum: not a clear indication unless related UTIs or bladder decompensation
- Medication failure: surgery recommended if bothersome symptoms persist despite maximal medical therapy
Choosing the right surgery
- Prostate size: prostates > 80-150g benefit from HOLEP or simple prostatectomy
- Anticoagulation: consider PVP/KTP, HoLEP to minimize bleeding
- Ejaculatory function: urolift, Rezum, and aquablation are more likely to maintain antegrade ejaculatory function postoperatively
- Median lobe: urolift less efficacious
- Prior prostate cancer treatment: prior cryotherapy or XRT increases risk for postoperative incontinence
- Laser type: KTP absorbed by Hgb, holmium/thulium absorbed by water
- Other considerations: risks/benefits, prior surgeries, surgeon experience, patient preference
- Workup: patient should undergo cystoscopy + sizing to assess best treatment option, can consider urodynamics prior to surgery if unclear cause of symptoms
- Incidental cancer diagnosis: if PSA < 4, cancer diagnosed in 1/382 TURPs (uncommon)
- See the separate page for technique info about TURP, UroLift, PVP, and TUIP
Large prostate surgery options
- Robotic simple prostatectomy (RASP): most invasive but most effective for retention treatment and symptom resolution
- HOLEP: risk of SUI, morcellation injury, long learning curvet
- Aquablation: water jet vaporization of prostate, 15% ejaculatory dysfunction and 0% stress incontinence, now w/ low transfusion rate (cauterize bladder-neck bleeding)
- Prostate artery embolization (PAE): 58% symptom reduction at 3-6mo, larger prostates have better outcomes, retention may take up to 3mo to resolve, 57% develop PAE syndrome (frequency, dysuria, pelvic pain), 16% retreatment at 5yr
Clinical scenario: patient with > 100g prostate, with(out) urinary retention, and no prior prostate cancer workup
- RALP may have increased risk for incontinence due to bladder neck reconstruction
- RALP age cutoff 70 (with exceptions), whereas RASP has no age cutoffs
- RASP + XRT may be better option for continence and prostate cancer than RALP
- MRI prostate, PSA, and biopsy will not change need for RASP (or other outlet procedure)
- Can perform biopsy at time of RASP
- Can consider XRT or other adjuvant therapies based on post-RASP PSA
- THEREFORE: in patient with 100+g prostate, can offer up-front RASP with truncated prostate cancer workup to avoid delaying treatment of urinary retention, but has risk of requiring XRT afterwards (difficult to perform RALP after RASP)
References
- AUA Core Curriculum
- Capogrosso, P., A. Salonia, and F. Montorsi. "Evaluation and Nonsurgical Management of Benign Prostatic Hyperplasia." Campbell-Walsh Urology 12 (2020).
- Helo, S., C. Welliver, and K. McVary. "Minimally Invasive and Endoscope Management of Benign Prostatic Hyperplasia." Campbell-Walsh Urology 12 (2020).
- Parsons, J. Kellogg, et al. "Surgical management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA guideline amendment 2020." The Journal of urology 204.4 (2020): 799-804.
- Wieder JA: Pocket Guide to Urology. Sixth Edition. J.Wieder Medical: Oakland, CA, 2021.