Prostatitis, Orchitis, and Epididymitis
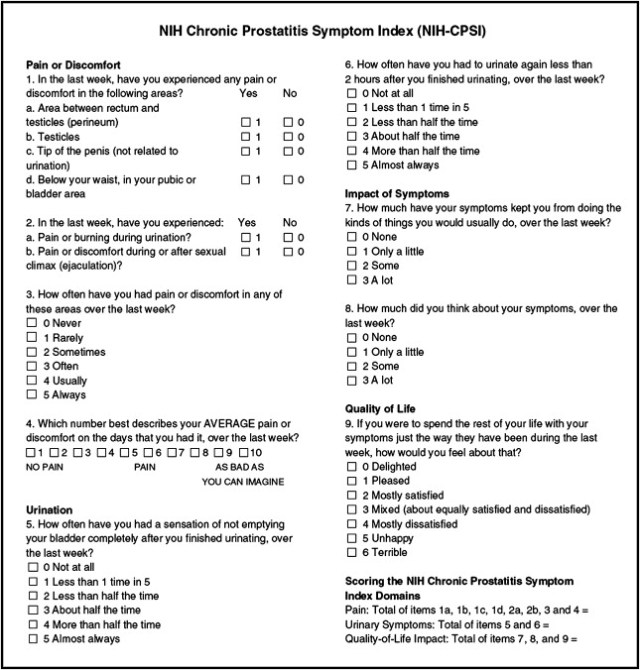
CPSI to assess prostatitis symptoms, from Litwin 1999
Bacterial prostatitis
Acute prostatitis (I)
- Histologic dx: presence of inflammation on prostate samples
- Clinical dx: UTI (frequency + dysuria) +/- systemic symptoms (fever, malaise, myalgias) +/- pain (lower abdominal or perineal)
- Exam: DRE ok, but prostate massage can cause sepsis, check PVR to rule out retention (consider placing SPT)
- Labs: UCx and CBC, consider blood cultures if systemic symptoms
- Treatment: 4-6wks lipid-soluble antibiotics, includes quinolones, trimethoprim, macrolides, tetracyclines
Chronic prostatitis (II)
- 2 glass test: urine culture obtained before and after prostatic massage, > 95% accurate for diagnosis
- 4 glass (Mears-Stamey) test: historic gold standard, collect initial 5-10mL voided urine, midstream urine, prostate massage expressed secretions, and post-massage urine
- Further workup: assess for retention (PVR), cancer (DRE), scrotal/abdominal exam, hematuria, consider sending for other cultures if history HIV or immunosuppressions, if < 45yo and first UTI, rule out urethral stricture with RUG
- CT imaging: obtain if UTI and hx DM, CKD, stones, LUTS, neurologic disease, hematuria, or urea-splitting bacteria
- Antibiotics: need to have good lipid solubility, includes quinolones, trimethoprim, macrolides, tetracyclines, may require treating for up to 6mo
- TURP: has been shown to improve symptoms in 52-67%
Chronic Prostatitis + Pelvic Pain Syndrome (IIIa+IIIb)
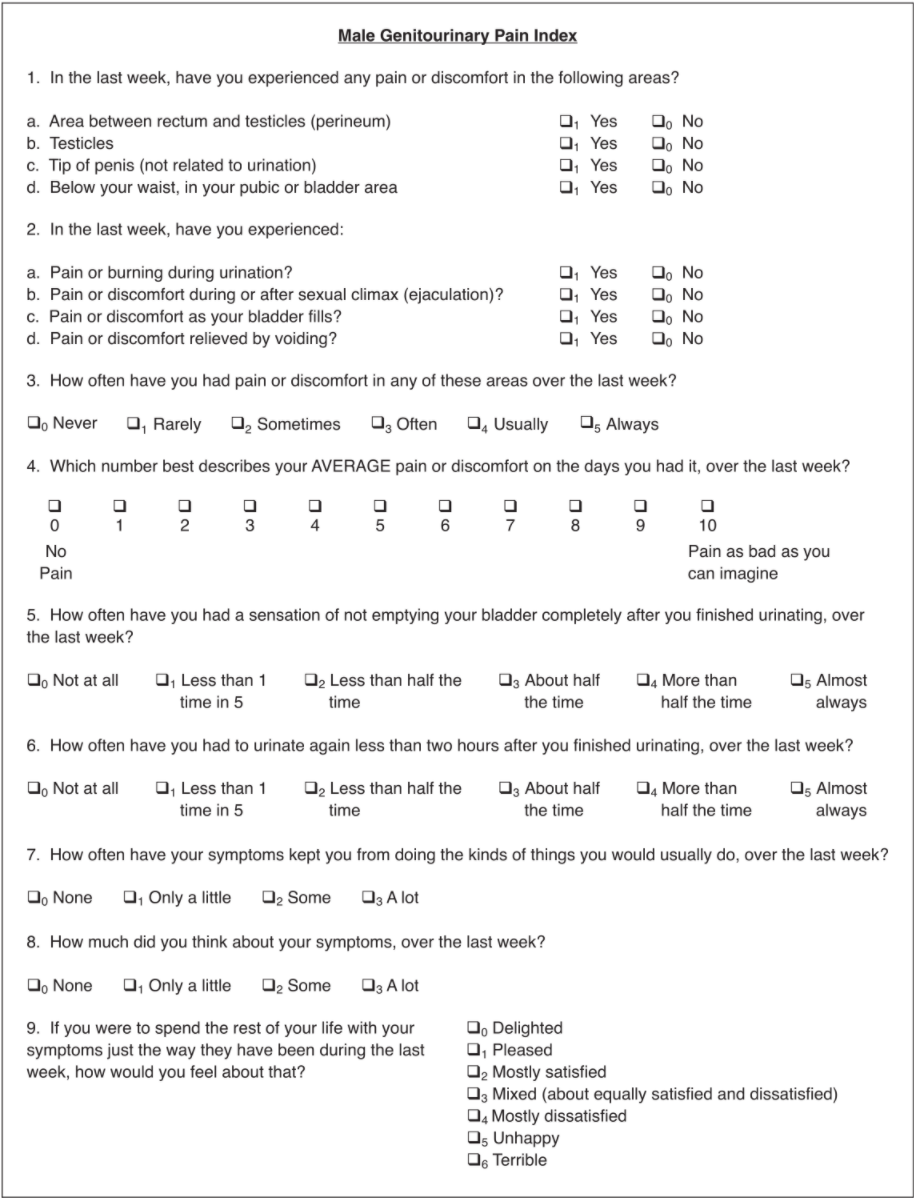
Pelvic pain index, from Clemens 2009
Potential causes
- Infection: may have history recurrent UTI
- Inflammation: histologic confirmation does not correspond with symptom severity
- Neurologic: patients demonstrate central sensitization (neural stimulation in absence of stimulus)
- Pelvic floor dysfunction: spastic pelvic muscles, difficulty relaxing, confirm on exam
- Psychosocial: association between pain and perceived stress
- Endocrine: higher levels cortisol may be present
- Genetic: association between CPPS and other pain conditions
Evaluation/Diagnosis
- Diagnosis of exclusion: pain in the absence of urethritis, GU cancer, UTI, strictures, or NGB
- Assess for nonurologic associated symptoms: GI, neuro, rheum (chronic pain syndromes)
- DRE: rule out acute prostatitis or prostate cancer, assess pelvic floor tenderness
- Other testing: obtain UA, UCx, PVR, consider cytology, PSA, imaging, cystoscopy
Treatment via "UPOINT" system (outdated)
- THE KEY: most of the below management plans indicate that "chronic prostatitis" is actually a mis-diagnosis and there is another underlying condition, most patients can likely be managed with "UPT" alone
- Urinary: alpha-blockers and 5ARi for voiding symptoms, pentosan polysulfate for bladder pain with filling (IC/BPS)
- Psychosocial: diet (food sensitivity), exercise, stress management
- Organ-specific: prostate massage, frequent ejaculation, circumcision, botox, TUIP
- Infectious: questionable benefit to antibiotic treatment, consider 6 weeks (quinolones/tetracyclines) if no prior antibiotic treatment and symptom duration < 1yr
- Neurologic: TCAs, gabapentin/pregabalin, SSRI/SNRIs, SNS/PTNS
- Tenderness (MSK): PFPT
- Other treatments: NSAIDs, quercetin 500mg BID (bioflavonoid)
Types of Prostatitis (in table form)
| NIH Classification | Symptoms | Pyuria? | Bacteruria? | Treatment | Key findings |
|---|---|---|---|---|---|
| Acute bacterial (I) | UTI symptoms Systemic (fever/chills) Pelvic pain |
Yes | Yes | PO/IV antibiotics x2-4 weeks 6mo if TB related |
Acute infectious + systemic symptoms |
| Chronic bacterial (II) | Recurrent UTIs | Yes | Yes, 10x increase after prostate massage | Antibiotics x4-6 weeks | Recurrent UTI with same organism |
| Chronic prostatitis/pelvic pain Inflammatory (IIIa) |
Pelvic pain without positive urine cultures | Yes (especially after prostate massage) | No | UPOINT | Pelvic pain in absence of infectious symptoms |
| Chronic prostatitis/pelvic pain non-Inflammatory (IIIb) |
No (even after prostate massage) | ||||
| Asymptomatic inflammatory (IV) | None | Yes | No | None | Discovered incidentally on biopsy/semenalysis |
Other prostatic infection
Prostate abscess
- Evaluation: suspect if prostatitis diagnosis and persistent fevers despite 48hrs abx
- Risk factors: catheter/GU instrumentation, DM, HIV, cirrhosis, ESRD/HD, BOO, prostate biopsy
- Imaging: confirm diagnosis with CT pelvis with contrast
- Management: if < 1-2cm, okay for antibiotics only, otherwise consider percutaneous drainage (recurrence rates 15-33%), if "very large" or abscess recurs, perform TUR unroofing
Post-prostate biopsy sepsis
- Initial treatment, carbapenems, amikacin, or 2nd/3rd gen cephalosporins, do not treat with bactrim or quinolones (high rates of ESBL resistance)
- Further treatment: can transition to quinolones if culture is sensitive, recheck culture in 1 week to confirm resolution
Granulomatous prostatitis
- Cause: commonly seen with TB infection or after BCG administration
- Histology: epithelioid granulomas
- Workup: check Tb cultures and acid fast staining of prostatic secretions or semen
- Treatment: only treat if symptomatic, isoniazid 300mg QD + rifampin 600mg QD x3-6mo, also give pyridoxine 50mg QD
IgG4 prostatitis
- Cause: may be seen with retroperitoneal fibrosis (Ormond disease)
- Histology: fibroinflammatory cells with IgG4+ plasma cells
- Treatment: responds well to steroids, consider in patient with LUTS and autoimmune pancreatitis/cholangitis, or histologic confirmation
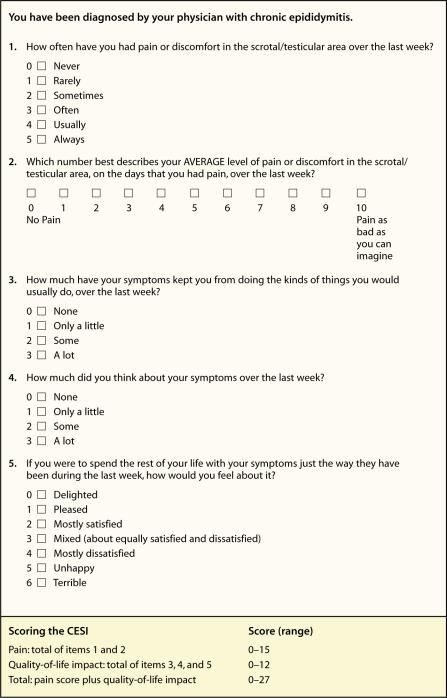
Chronic epididymitis evaluation scale, from Nickel 2003
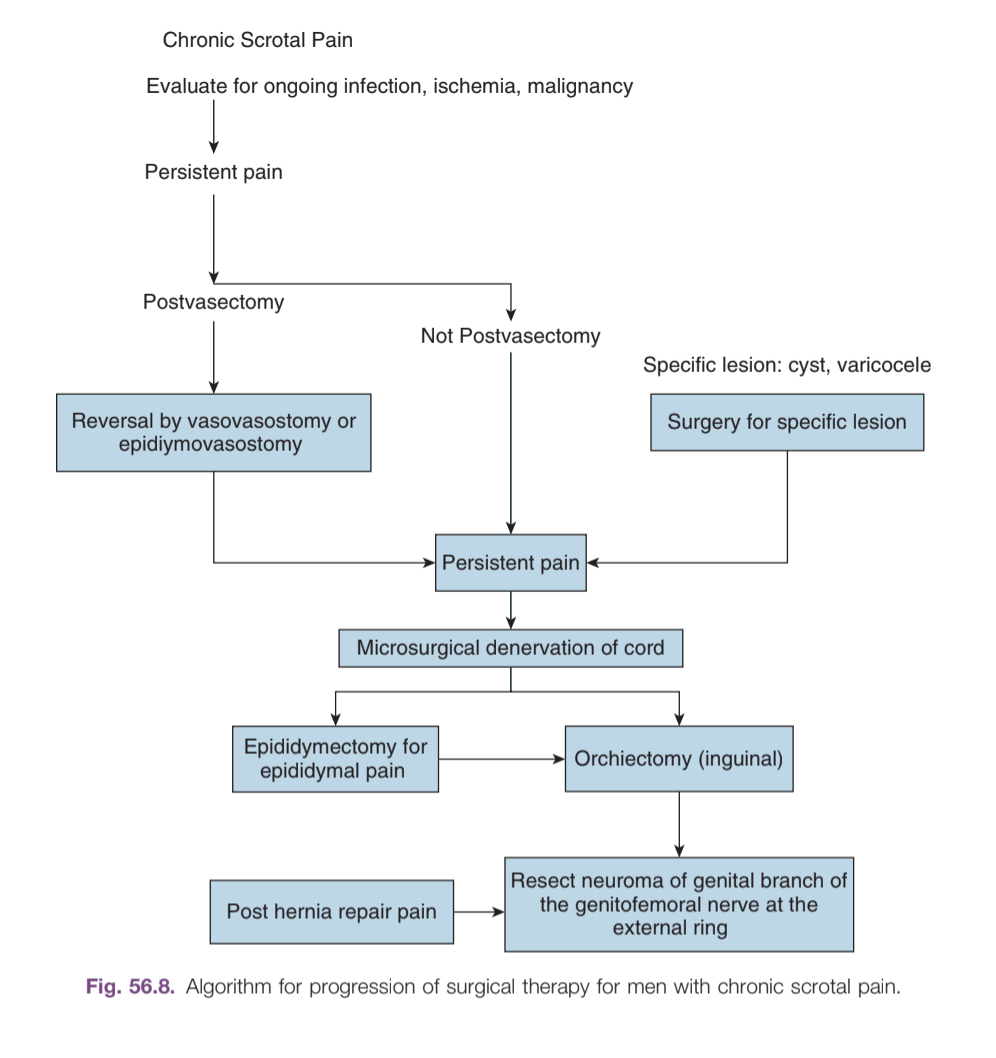
Algorithm for management of chronic scrotal pain, from Campbell's
Epididymoorchitis
Acute epididymoorchitis
- Non-infectious causes: tumors, Behcet disease (oral/genital ulcers, uveitis, skin lesions), amiodarone epididymitis, anti-sperm antibodies, trauma, torsion
- Infectious causes: E. coli, gonorrhea, chlamydia, mumps, coxsackie virus, Tb, fungus, ureaplasma, Trichomonas
- Potential symptoms: pain, swelling, urethritis/discharge, fever, hydrocele, erythema/edema on exam
- Workup: diagnosis and underlying cause made with history/physical, scrotal US can be beneficial but not required if diagnosis clear
- Infectious treatment: ceftriaxone 250mg IM x1 + doxycycline 100mg BID x10 days (if STI suspected), levofloxacin 500mg daily x10 days (if UTI suspected), ceftriaxone 250mg IM x1 + levofloxacin 500mg daily x10 days (if cause unclear)
- Further management: admit for IV antibiotics if fevers or leukocytosis, consider repeating imaging if no improvement within 72hrs, induration/swelling can takes weeks/months to resolve
Chronic epididymoorchitis
- Definition: pain lasting for > 6 weeks
- Causes: post-surgical, pelvic floor dysfunction, post-infectious, granulomatous, amiodarone, tumor, varicocele, referred pain (stone, hernia, herniated disc, aortic aneurysm), may be idiopathic (18-25%)
- Post-vasectomy: 30% report short-term pain, chronic pain in 0.1-15%
- Granulomatous: can be infectious (TB, brucellosis, syphilis, leprosy), post-BCG, sarcoidosis, or idiopathic, may require orchiectomy to differentiate from malignancy
- Workup: culture urethral discharge (if present), scrotal US (assess for testicular abnormalities), can consider CT imaging to assess for causes of referred pain
- Conservative management: scrotal support, NSAIDs, avoid exacerbating activities, heat/ice packs
- BCG orchitis: isoniazid 300mg QD and rifampin 600mg QD x3-6mo, check LFTs and give Vitamin B6 50mg QD while taking isoniazid, do not need to treat if asymptomatic
Minimally invasive therapies
- Pelvic floor PT: consider if abnormal pelvic floor tone is noted on DRE and patient has other associated symptoms
- Cord block: inject 20mL 0.25% bupivicaine (without epinephrine) into spermatic cord, can also combine with methylprednisolone, resolution of pain indicates non-referred pain and cord denervation may be beneficial, testicular atrophy is rare but possible side effect
- Botox: inject 100U distal to external ring, wears off by 6mo
Surgical options
- Targeted excision: if pain is clearly due to hydrocele, spermatocele, torsion, patients report good improvement with repair
- Varicocelectomy: microsurgical (up to 85% pain resolution), nonmicrosurgical (up to 72%)
- Post-vasectomy pain: pain may be due to sperm granuloma, consider vasectomy reversal, may take 3mo to improve pain
- Cord denervation: transect nerves found in cremasteric muscle fibers, perivasal sheath, and posterior lipomatous tissue (trifecta nerve complex), cure rates 50-70%
- Neuromodulation: minimal data, only effective with case reports
- Epididymectomy: complete improvement in 50-75%, progression to orchiectomy in 22-100%
- Orchiectomy: relief in 0-75%, better improvement with inguinal approach
- Post-orchiectomy phantom pain: identify genital branch of genitofemoral nerve, resect neuroma, place proximal end into pelvis