Urologic Tubes
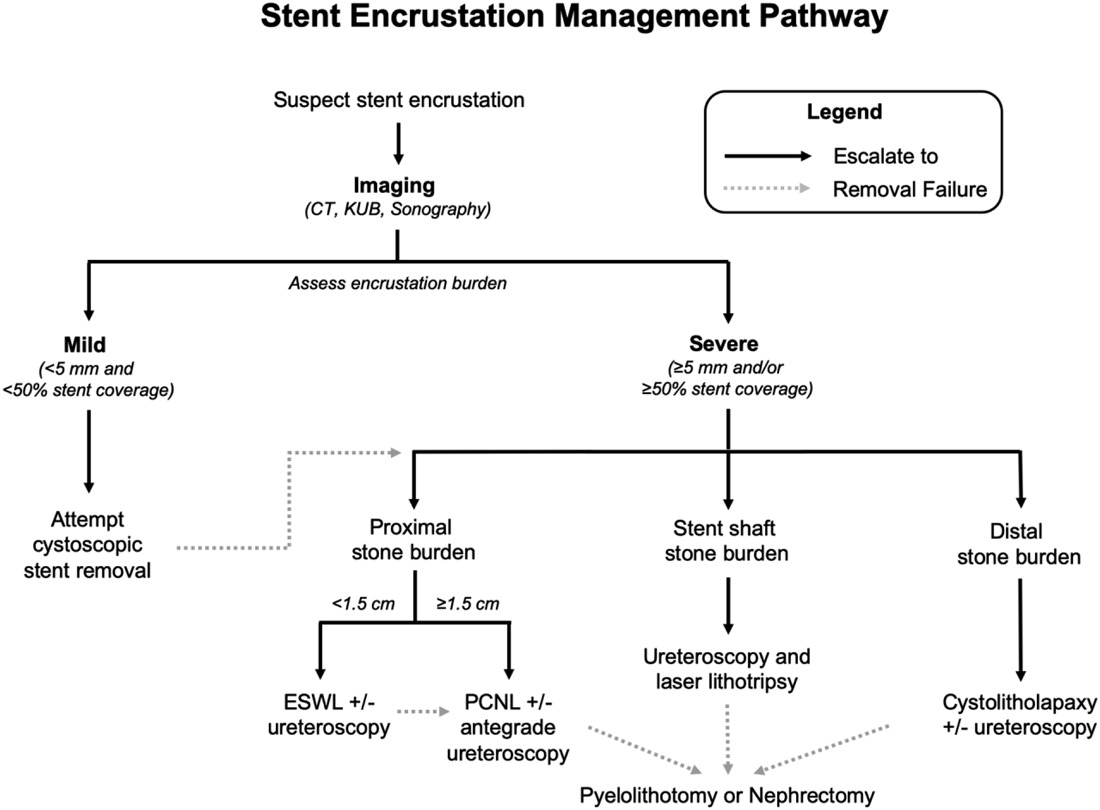
Management of stent encrustation, from Tomer 2021
Upper Tract Drainage
Nephrostomy tubes (PCNs) and percutaneous access
- Indications: bypass obstruction, diagnostic studies, instill chemotherapy, postsurgical drainage
- Percutaneous access: safest via papillary approach due to lack of vessels, although some evidence that infundibular approach has no increased bleeding risk
- Anticoagulation: need to stop prior to access, although aspirin use does not seem to increase bleeding risk
- Ribs: entry above 11th rib has high risk for pleural injury, entry above 10th rib has high risk for lung injury
- Blind access: access via Grynfeltt lumbar triangle - borders are 12th rib, quadratus lumborus, transversus abdominis, and internal oblique, insert needle 3-4cm at 30degree cephalad angle
- Nephroureteral stent: consider if concern that tube will become dislodged with movement
- Options: cope loop (pigtail secured with string), council catheter placed over wire, Malecot catheter placed with straightener, or nephroureteral stent
- Complications: acute bleeding requiring transfusion (0.5-4%), delayed hemorrhage (< 1%), perforation, colon injury (0.1%), splenic/hepatic injury (less rare if access is above 10th rib), hydrothorax/pneumothorax (rare if access below 12th rib), urinothorax (2% if access above 12th rib, 6% if access above 11th rib)
Ureteral Stents
- Indications: infection and obstruction of upper tract, malignant obstruction
- Placement: fluoroscopically (marker over pubic symphysis), under direct visualization, or by feel (female only)
- Floated stent: distal stent tip pushed within ureteral orifice, can attempt removal with basket or ureteroscopic graspers, occasionally needs to be removed percutaneously
- Stent pain: manage discomfort with a-blockers, NSAIDs (preferred over opioids), and antimuscarinics
- Encrustation occurs in up to 13%, increased risk with diabetes, rUTI, renal failure, pregnancy, manage depending on severity and location of encrustation
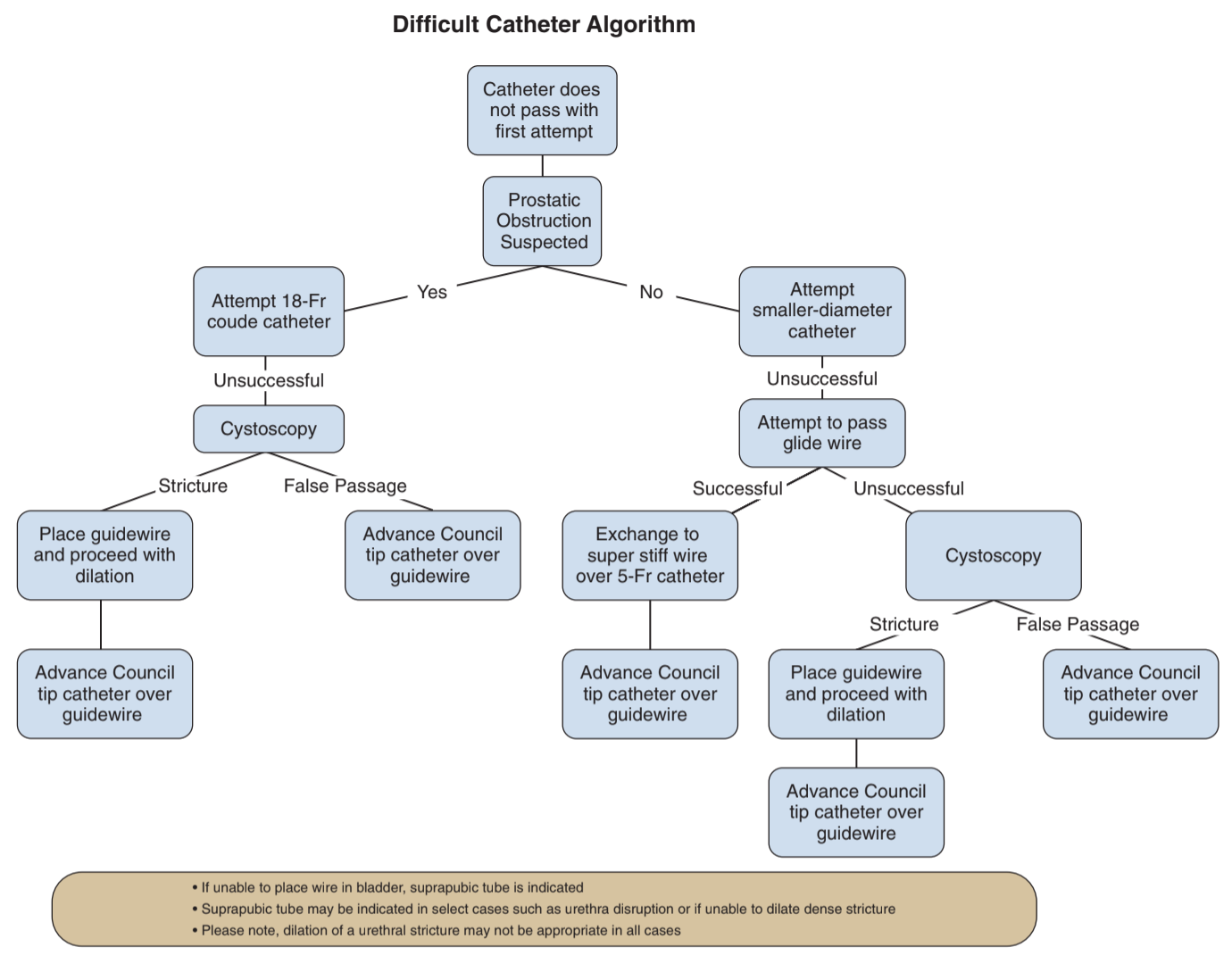
Difficult catheter algorithm, from Campbell's
Lower Tract Drainage
Catheter types and indications
- Coude: upwards curve helps maneuver prostate, larger size (18+) better otherwise catheter will buckle
- Silicone: stiffer catheters help navigate strictures and blind placement with severe phimosis, smaller size (12Fr) works best
- Council: hole at tip to pass over wire after dilating urethral stricture
- Rusch: stiffer material allows for irrigation of large clots without collapsing during aspiration, 3-way for continous bladder irrigation
Placement tips
- Relaxation: taking slow deep breaths in via nose out via mouth helps relax sphincter and makes placement easier
- Lubricant: injecting directly into meatus improves placement but may initially clog drainage hole (need to flush)
- Lube temp: cooling in cup with ice helps decrease discomfort
- Hubbing: ensure hubbed completely prior to inflating balloon (avoids inflating in prostatic urethra)
- Urine level: if air/fluid level moves with patient respirations, catheter is adequately placed in bladder
- Female position: trendelenberg, frog-leg, pillow under hips, retract labia up and outwards
- Female urethral identification: under pubic bone (retracts into vagina with aging), can blindly slide catheter over finger in vagina, coude may help
Difficult situations
- History: assess prior abdominal surgeries, urethral stricture disease, prior prostatic/bladder surgeries
- BPH: use coude, larger sizes pass more easily (18Fr > 12-14Fr)
- Stricture/phimosis: use silicone (stiffer), smaller size (12-14Fr), can blindly place through foreskin into meatus
- Concern for false passage: have concern if no urine return or blood at catheter tip, may require cystoscopy, false passage usually posterior and true lumen more anterior
- Difficult stricture: attempt placement of open ended catheter and wire, otherwise visualize stricture directly with cystoscope, then use dilators (straight or S-shaped) over stiff wire before placing Council, dilate 2 sizes greater than catheter, council catheter may not be stiff enough (use silicone with hole punched in end)
- Buried penis: pressure on surrounding tissue exposes penis, otherwise may have to place blindly or use cystoscope to identify meatus
- Posterior valves: use 5Fr anteriorly-curved catheter, can place finger in rectum to guide catheter if necessary
- Continent reservoir/pouch: overdistention may cause channel to kink, use cystoscope/ureteroscope to place guidewire, leave catheter for 1-2 weeks to heal
- Ileal conduit: can place catheter past stoma and inflate halfway, may need to secure to skin with stitch
- Artificial sphincter (AUS): avoid catheters if possible, place 12Fr if needed and remove as soon as possible to avoid erosion
- Difficult female catheters: place bed in trendelenberg and put pillow under hips to anteriorly elevate/tilt pelvis, have assistant retract labias laterally and anteriorly, can use coude to catch retracted urethral meatus, can place blindly over finger in vagina (will feel anterior vaginal wall between properly placed catheter and finger)
Post-obstructive diuresis (POD)
- Definition: UOP > 200mL/hr x2+ hrs or > 3L/d after removal of GU tract obstruction
- Physiologic diuresis: release of water/salt overload, resolves spontaneously
- Pathologic diuresis: continued high UOP due to loss of ADH feedback
- Hematuria: develops in 10% after relieving retention, may occasionally require clot irrigation
- No evidence/benefit to catheter clamping to prevent hematuria or POD
- Admit patient if AKI, electrolyte imbalance, or neurologic symptoms - monitor electrolytes
- If patient able to tolerate PO intake, regular salt/water balance with PO fluids
- If patient unable to tolerate PO intake, replete with 0.9% or 0.45% saline, repleting 50-80% UOP losses (avoids persistent fluid overload)
- Intermittent clamping: no proven benefit to intermittent clamping in RCT (Boettcher 2013), risk for hematuria is rare
Chronic Catheterization
Intermittent Catheterization (CIC)
- Avoids UTI, which are caused by overdistension and retained urine, not bacteruria
- Patient/caregiver needs to be able to perform
- Can be clean, aseptic, or sterile, can rinse, wash with soap, boil, or microwave
- Maintain bladder volumes < 400-500mL
- Infection prevention: consider nightly instillation of 50mL 2% betadyne or antibiotic solutions (480mg gentamicin in 1L NS, instill 30mL)
Longterm catheterization
- Consider when unwilling/unable to perform CIC and unable to adequately empty bladder
- SPT has lower risk for UTI, epididymitis, and urethral stricture, allows preservation of sexual function
- Bladder cancer risk 8-10%, recommend annual cystoscopy starting 5-10yrs after catheterization begins
- Purple bag syndrome: indoxyl sulfate (tryptophan metabolite) excreted in urine, bacteria with phosphatase/sulfase enzyme (rare) convert it to blue/red colors, concentrated in tubing and bag creating purple/blue bag, more common in constipated and elderly patients
Suprapubic tubes
- Indications: urethral obstruction/stricture, urinary retention, longterm neurogenic bladder management
- Avoid placement if overlying bowel or prior pelvic surgeries (can confirm with CT pelvis), hx bladder cancer (concern for tract seeding), or anticoagulated
- Benefits: easier to change, easier to manage, allows for sexual activity, 89% patients prefer SPT over prior urethral catheter, no difference in UTI risk but decreased risk of prostatitis/epididymoorchitis, decreased risk of urethrovaginal fistula or traumatic hypospadias
- Placement techniques: can use punch trocar, dilating trocar over wire, or cope loop over wire
- Lowsley retractor: modified urethral sound, place into bladder and push up against abdominal wall then incise down onto retractor, grasp catheter and pull into bladder
- If high risk for bowel injury, can place via cut-down technique
- Placement complications: bleeding (2%), infection (9%), malposition (3%), bowel injury (2.5%), mortality (0.8-1.8%), ureteral obstruction (rare), bladder perforation (rare)
Common catheter complications (urethral and suprapubic)
- Acutely not draining: check bladder scan (may not be draining), flush to remove debris/clots, ensure flushes/aspirates, consider replacing catheter (ensure placement in bladder)
- Chronic clogging: exchange tube monthly or more frequently, consider daily/BID saline flushes, can consider renacidin irrigation, maintain fluid intake (dilute urine), consider citric-acid containing beverages to acidify urine (prevents precipitation in alkaline urine), consider cystoscopy or ultrasound to assess for bladder stones (may not show up on XR), minimal benefit to upsizing catheter
- Peri-catheter leakage: confirm tube is draining, consider anticholinergics, avoid upsizing (stretches out SPT tract)
- Bladder infections: only treat if clinically significant (do not treat asymptomatic bacteruria), exchange tube more frequently, consider CIC, consider methenamine
- SPT discharge: greenish discharge may be local S. aureus infection, no treatment required but can manage with daily betadyne wipe, granulation tissue can be treated with silver nitrate swabs
- Bladder stone: usually secondary to UTI and stasis, seen in 40-50% catheter blockages
- Erosion: irreversible, traumatic hypospadias seen in men (no treatment required), bladder neck erosion with urethrovaginal fistula seen in women (requires closure or PVS to prevent persistent leakage with SPT placement)
- Unable to remove: can cut balloon port (may be malfunctioning), inject mineral oil and wait 5-10min (helps loosen balloon), try to remove with gentle traction (balloon may not be 100% deflated but will come out), can try popping with superstiff wire via balloon port, do not overinflate (can leave balloon parts in bladder), can puncture via suprapubic route (male) or transurethral/vaginal route (female) under ultrasound guidance, may require surgical removal if large encrustation on catheter
Condom catheters
- Option for patients with poor mobility and/or incontinence and otherwise able to completely empty bladder
- Lower rates of UTI and death compared to indwelling catheter, better QoL
- UTI risk increases if catheter not changed daily
- Complications: allergic reactions, skin maceration/breakdown, penile edema, rarely cause pressure necrosis and urethral injury
- Can consider malleable penile prosthesis placement to prevent device from falling off, 5% infection rate, 8% explant rate
References
- AUA Core Curriculum
- Boettcher, S., et al. "Urinary retention: benefit of gradual bladder decompression-myth or truth? A randomized controlled trial." Urologia internationalis 91.2 (2013): 140-144.
- Boone, T., J. Stewart, and L. Martinez. "Additional Therapies for Storage and Emptying Failure." Campbell-Walsh Urology 12 (2020).
- Daneshmand, Siamak, David Youssefzadeh, and Eila C. Skinner. "Review of techniques to remove a Foley catheter when the balloon does not deflate." Urology 59.1 (2002): 127-129.
- Dauw, C. and J. Wolf. "Fundamentals of Upper Urinary Tract Drainage." Campbell-Walsh Urology 12 (2020).
- English, Sharon F. "Update on voiding dysfunction managed with suprapubic catheterization." Translational andrology and urology 6.Suppl 2 (2017): S180.
- Jacob, J. and C. Sundaram. "Lower Urinary Tract Catheterization." Campbell-Walsh Urology 12 (2020).
- Jane Hall, Susan, et al. "British Association of Urological Surgeons suprapubic catheter practice guidelines–revised." BJU international 126.4 (2020): 416-422.
- Tomer, Nir, et al. "Ureteral stent encrustation: epidemiology, pathophysiology, management and current technology." The Journal of Urology 205.1 (2021): 68-77.
- Villanueva, Carlos, and George P. Hemstreet III. "The approach to the difficult urethral catheterization among urology residents in the United States." International braz j urol 36 (2010): 710-717.
- Wieder JA: Pocket Guide to Urology. Sixth Edition. J.Wieder Medical: Oakland, CA, 2021.